




What are the uterine fibroids?
Uterine fibroids are common, in the vast majority benign, tumors of the uterine muscle (myometrium). The rule of thumb is they require treatment when, due to their size or location, they cause symptoms. It may also be preferable to consider treating them before attempting a pregnancy, aiming to:
- improve fertility
- reduce the risk of complications during pregnancy and labour (fibroid necrosis – pain, premature birth, bleeding)
Commonly, uterine fibroids are incidental findings during a routine gynaecological examination.
How do uterine fibroids relate to estrogens?
Uterine fibroids are hormone-dependent tumors and grow under the influence of estrogen. Pre-menopausally, estrogens are mainly secreted by the ovaries and are also a component of preparations such as the combined contraceptive pill and hormone replacement therapy.
After menopause, in the absence of estrogen, any pre-existing uterine fibroids usually stabilize in size and regress in the long run. This process is expected to be slower in women:
- receiving hormone replacement therapy
- are obese as adipose tissue is a source of conversion of normal adrenal-produced androgens to estrogen
The Gynaecologist Surgeon Dr. Christina Founta has years of experience in diagnosing and treating women with uterine fibroids in the UK, as a member of Gynaecological Oncology teams of large British hospitals. She is performing a full range of complex operations for uterine fibroids, both laparoscopic and . She is a member of the Gynaecological Oncology team of ‘Mitera’ Hospital of the ‘Hygeia’ Group and undertakes the full range of gynaecological operations listed below.
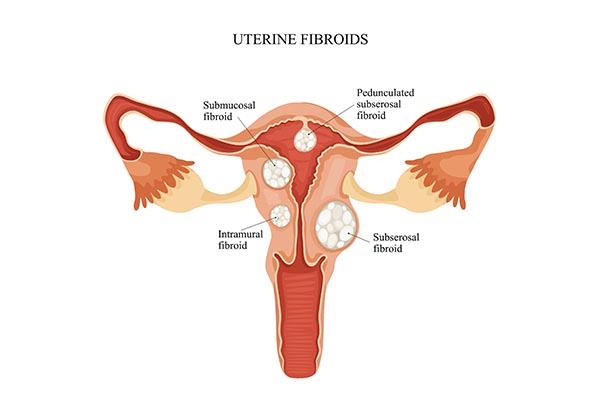
How are uterine fibroids classified?
Uterine fibroids are classified according to their position in relation to the myometrium. This classification is of particular importance as it determines the probability and type of symptoms as well as the appropriate methods of treatment.
Submucosal uterine fibroids
Submucosal fibroids are located inside the wall of the uterus and protrude fully or partially into the endometrial cavity.
Uterine submucosal fibroids are the most likely to cause symptoms, with more frequent the bleeding between periods that can vary in severity. In addition, due to their location, they can cause problems such as:
- infertility
- miscarriage
- abnormal location of the placenta
- placental abruption
- bleeding during pregnancy and labour
Submucosal fibroids often need to be removed. In most cases, hysteroscopic removal is the appropriate treatment for submucosal fibroids. It is performed transvaginally as a day surgery and is a minimally invasive method with very little risk of complications when performed by an experienced gynaecologist.
Intramural uterine fibroids
Intramural fibroids are located within the muscle of the uterus (myometrium). The most common symptom of intramural fibroids is heavy periods. This is a result of the reduced ability of the myometrium to contract in order to adequately control blood loss due to the presence of fibroids within it.
If the fibroids reach close to the endometrial cavity, they often also cause out-of-period bleeding and/or an irregular cycle. If they are large in size (usually over 5-6 cm) and/or multiple, they can cause symptoms of pressure such as:
- bloating
- increased frequency of urination
- constipation
- pain during sexual intercourse
- swelling of the lower extremities
- discomfort
- early satiety
- Shortness of breath
They can also increase the risk of thrombosis due to pressure onto large blood vessels. When uterine fibroids reach a large size, they may degenerate and cause pain.
If pregnancy is desired, large uterine fibroids must be treated surgically before attempting. Large fibroids can both cause infertility and are also associated with serious complications during pregnancy such as:
- first and second trimester miscarriages
- premature birth
- abnormal location of placenta
- bleeding during pregnancy and labour
- fibroid degeneration
- pain
However, if uterine fibroids are small in size (up to 2-3 cm), the risk of causing problems during pregnancy pregnancy is very low.
Intramural uterine fibroids: Management options
When uterine fibroids are small and asymptomatic with benign features and without rapid increase in size and morphology, simple monitoring is recommended. This includes clinical evaluation/examination and ultrasound examination. On indications and to answer specific diagnostic questions, MRI can also be used. The frequency of follow-up is individualized according to the characteristics of the specific woman.
Surgical treatment
This comprises of either removing the fibroid/s (myomectomy) with preservation of the uterus or hysterectomy, with or without removal of the ovaries. The decision for the appropriate intervention depends on the following factors:
- the size of the fibroids
- their characteristics
- the age of the patient
- the desire for future fertility
- patient preference
Most operations for benign fibroids can be performed laparoscopically, especially myectomies. Many hysterectomies are also performed laparoscopically, as long as the ratio of the uterine volume to the total volume or peritoneal cavity volume permits the necessary manipulations. Surgery has the most immediate results and is the appropriate method for women who wish for a future pregnancy. It has the disadvantage that it is a major surgery, but in the right hands it is extremely safe. Women with a history of myomectomy may be considered safer to give birth by caesarean section (C-section), which is necessary if the endometrial cavity has been breached during surgery.
Uterine artery embolism
It is an interventional radiology method with the aim of reducing the blood supply to the uterus, and consequently to the fibroids, leading to their shrinkage. It is not suitable for women who want to have children. It has the advantage that it is less invasive than surgery. The disadvantages of this method are:
- results take longer to be achieved
- possibility of not working as well as expected
- uterine fibroids often degenerate with accompanying pain and risk of infection
Medical management
It is possible to administer medication which cause temporary menopause and help shrink uterine fibroids. These are usually used before surgical removal to make it technically easier and reduce the risk of complications such as bleeding. In young women whose periods return after discontinuation of treatment, the fibroids are likely to reoccur if they are not removed.
Subserosal uterine fibroids
Subserosal fibroids are located on the outer surface of the uterus. Typically, the symptom caused by subserosal uterine fibroids is pressure on the surrounding organs if and when they grow in size. The treatment methods are the same as for intramural uterine fibroids. Technically, surgical removal is usually easier and is associated with a lower risk of intraoperative and postoperative complications.
Malignant transformation
The transformation of fibroids into malignant tumours (leiomyosarcoma) is very rare. They appear as solitary tumours with rapid growth in size, increased vascularity and atypical features. These are aggressive malignancies that need to be treated by a Gynaecologic Oncologist and a specialized team.
Finally, STUMP (uterine Smooth muscle Tumour of Unknown Malignant Potential) is the term characterizing myometrial tumours that are neither categorized as benign fibroids nor as malignant leiomyosarcomas. The final diagnosis is made histologically after removal, and the suspicion is set through preoperatively imaging. The appropriate treatment is hysterectomy, especially in cases where childbearing has been completed. It is important for the operation to be performed by a Gynaecologist Surgeon with experience in Gynaecological Oncology after discussion in gynaecological oncology MDT meeting. Once removed, these tumors have excellent prognosis.

